Physicians
have been largely silent on two
nuclear industry challenges before the federal government. Do
we pour millions of dollars into research and development of Small
Modular Nuclear Reactors? Do
we bury our current nuclear waste in the vicinity of Wakerton,
Teeswater and Kincardine and
the city of Ottawa in
Ontario?i
In
fact, physicians have been silent about nuclear power in general. We
have also been silenced as the industry has worked its mysterious
media fantasy of “too cheap to monitor” into a myth of
“necessity” for climate change energy. We have been silent, not
because we have nothing to say but because we’ve been led to
believe that these decisions are “political”, not health-related.
During
the Canadian Covid epidemic, physicians were utterly unable to keep
the primacy of health care out of the political arena. We saw our
ICUs worked beyond capacity, and our colleagues quit in frustration.
With respect to the threat of ionizing radiation we have been
remarkably silent.
To
reiterate, the two very different questions currently before Canadian
legislators, both involve ionizing radiation, not merely that of
nature (sun, rocks, air) but entirely man-made atoms, some of which
will still be emitting ionizing radiation in a time-frame that is
outside human comprehension (plutonium-239 will be around for 24,100
x 10 yearsii).
1.
Nuclear Waste Management:
Having
decided that the only way to “manage” nuclear waste was to put it
into a Deep Geological Repository (DGR),
the
Nuclear Waste Management Organization (NWMO)iii
has spent the last two
of decades
searching
for such a site.
The
process has divided communities even while much of negotiation with
perceived leaders (mayors, chiefs and council members) has occurred
behind closed doors. Health
professionals have been silent.
These
wastes will be toxic for a long, long time. They are not like
ordinary waste simply degrading over time. Each nuclear element has
its own decay chain. What is buried in 2030 will never
be what it
was
again.
Short-lived
waste and decay products will disappear
but
longer-lived ones will continue to emit radioactivity. A
cask of nuclear waste is like a boiling cauldron with atoms of
ever-changing elements.
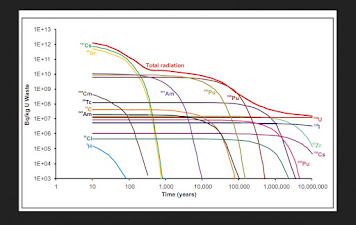
From this graph, you can see that the total radiation has decreased over 10 million years.
While
it is easy to understand that burying the waste in undisturbed
bedrock changes the bedrock to a “disturbed” status, many
people don’t know that the radioactivity of the waste can change
the very containers in which they are buried. Refurbishing of nuclear
reactors involves replacement of miles of metal
pipes
that have become corroded, why would we expect that containers in a
DGR would fare better?iv
DGR?
This
is not the only disposal in question
– NWMO is
fantasizing
a Near Surface Disposal Facilityv
(NSDF) at Chalk River only 200 km North of Ottawa. This proposed
disposal facility would
be
an eight story mound that will be within a few hundred metres of the
river from which Ottawa and Montreal draw their cities’ drinking
water.
vi
From
Ionizing
radiation
directly affects the human genome. No
one disputes this but many believe or pretend to believe (denial)
that there is a low level at which it is actually beneficial.
Hormesis
is
a fiction.
Physicians
often find themselves at odds with an industry when, using the
precautionary principle, we hesitate to approve a new drug or
technical procedure. For example, thalidomide’s disastrous side
effects became evident only after marketing. Our history with
radiation in medical use has been a continual story of overuse
followed by rationalizing behaviour.
A
radiological example, X-rays and CT scans. The overuse of x-rays for
removal of skin lesions led to discipline by the American Medical
Association at the end of the 1920’s and use for hair removal
forbidden. Using x-rays to treat Tinea capitus in Israel
resulted in a significant increase in cancers of the head and neck
decades later.
In
1996, I joined the multitude of physicians using CT scans “to rule
out brain injuries” in children that had bonked their heads – a
negative result tended to reassure both the parents and myself, only
to discover that these investigations resulted in an increase in
cancers years later.vii
Choosing Wisely, a program to guide physician decisions about
lab and x-ray investigations, now recommends CT scans under a limited
number of circumstances – none of which are “I want reassurance”
or the “parents expect it.
The
industry has settled upon a Deep Geological Repository (DGR). What
could be simpler? Bury it deeply in the bedrock where it would be
safe and immobile for time immemorial. Are we so brilliant and so
prescient that we can know what will be safe for the next 100,000
years and more?
Currently
the waste is stored in concrete containers above ground. They can be
watched – providing jobs for generations of Canadians – and
repackaged if they leak. “Rolling Stewardship” would provide
laboratories in Canada and elsewhere with experimental material.
Finally, perhaps our brighter descendants will discover a way to use
ionizing radiation safely. Instead of choosing a DGR recklessly with
our limited understanding of the waste, we have the opportunity to
spawn years of research.
2.
Building Small Modular Nuclear Reactors:
Full
page ads about Small Modular Nuclear Reactors tout them as “safe”.
How is anything that produces ionizing radiation safe? We use it
extensively in diagnostics and treatment but we also know that it is
implicated in causing cancer.
In
the 1950’s we routinely x-rayed pregnant women for “pelvimetry”,
measuring their bony pelvic outlet to ascertain whether they could
give birth naturally or needed a Caesarian section. In both the USA
and the UK, the cancer societies noted a rise in leukemia in
children. Suddenly there was a boom in building pediatric hospitals
devoted to treating cancer.
During
the 1940’s and 1950’s, there was a leukemia boom in North
Armerica and the UK. There was a sudden increase in incidence from ~
1:20 to 1:16 children. At that time it was almost always fatal.
Dr.
Alice Stewart, a general practitioner in the UK and one of the first
epidemiologists, and the Tri-State Health Study in the USA collected
data and connected the dots. X-rays
during fetal development doubled the incidence of cancer in the
offspring. Doctors had
been ordering x-rays to measure womens’ pelvises, a series called
“”pelvimetry”. The technique disappeared. Lead aprons came out
for dental x-rays.
In
2007, after decades of study and six reports, the Biological Effects
of Ionizing Radiation (BEIR VII)viii,
in publishing its seventh report concluded that any level of exposure
to radiation was unsafe (although “at lose doses, the number of
radiation induced cancers is small”).
Studies
of significant increases in leukemia and other cancers within 5 to 25
km of operating nuclear power plants seem to yield conclusive results
but research by both the Committee on Medical Aspects of Radiation in
the Environment (COMARE, UK) and the Kikki
study in Germany have had disputed by the nuclear industry.
iP.
Kaatsch, C.Spix, S. Schmiedel, R. Schulze-Rath, A.Mergenthaler, and
M. Blettner, Epidemiologische Studie zu Kinderkrebs in der
Umgebung vonKerkraftwerken (KiKK Studie), Sltzgitter:
Bundesamp fuer Strablenschutz, 2007,
urn:nbn:de:0221-20100317939.
In
2012, I mentioned the German study in discussion after delivering a
brief to the Canadian Nuclear Safety Commission (CNSC). The health
science person on the board dismissively called the effect “due to
a virus.” If there is a special virus that affects only children
close to nuclear power plants, we should endeavour to identify it. No
such research appears to have been launched.
Before
1990, when it was forced to open its records, the United States
Department of Energy not only controlled access to all information on
the health effects of radiation on nuclear workers and the public but
it also controlled all the funding of radiation researchx.
It had successfully stone-walled independent research for decades.
We
don’t know which ray or particle will cause any particular DNA
molecule to turn the cell into cancer but we know that they do.
Physicians have conducted studies on the medical uses of ionizing
radiation. Here are a few examples:
a) Xray
treatment of Tinea capitus:
The
studies on patients who, as children, received x-ray treatment for
Tinea capitis (fungal infection of the scalp) in the 1940’s and
1950’s have shown “excess incidences of tumours of the head and
neck including the skin, brain, thyroid, and parotid glands”xi.
Needless to say, this technique of treating fungal infections is left
in the dustbin of history.
b) Breast
cancer after fluoroscopic examinations of the breast during treatment
for pulmonary tuberculosis:
“The
role of ionizing radiation as a cause of carcinoma has long been
recognized, particularly in relationship to carcinoma of the skin,
lung, thyroid and bone.”xii
Dr. Ian Mackenzie in Halifax found fifty cases of breast cancer in
patients who had received this form of x-ray treatment prior to 1961.
From length of time from the beginning of the x-ray treatments and
the breast cancer averaged 17 years. There was also a high
correlation between the side of treatment and the cancer-affected
breast.
This
method of treating pulmonary TB had disappeared by 1955 when
antibiotics became available but This research carried out largely on
indigenous women and largely had disappeared by 1955. Decades later
when they developed breast cancer, I’m sure they were very grateful
that they had contributed to show that breast tissue was sensitive to
radiation. Should we take a closer look at the use of x-rays in
mammograms?
c)
PET, MUGA, MIBI and SPECT scans:
All
of these scans use a radioisotope, an element that gives off gamma
rays that can create images of various parts of the body. For
example, I131 concentrates within 15 minutes in the thyroid. This can
provide a very good picture of the thyroid. Some studies require two
scans, one before the radioisotope is injected and then a later one
showing where the element accumulates in the body.
In
2011 researchers in Montreal examined the charts of more than 80,000
patients who had received post-heart attack PET scans and concluded
that there was a 3% increase in the incidence of cancer per 10 mSv of
scan exposurexiii.
Scans require between two and 8 exposures to satisfy the demands of
the test. (For comparison, 10 mSv is equivalent to the exposure from
100 chest x-rays).
d)
Increased secondary cancers in post-radiation patients:
“Radiation-induced
second malignancies (RISM) is one of the important late side effects
of radiation therapy”.xiv
The exact risk is dependent
upon so many factorsxv
that it probably contributes
only 5% increase
of the 17 – 19% total secondary cancers.
What
is quite amazing is the real paucity of good prospective research on
the health effects of radiation. These ones briefly listed here
concentrate on carcinogenic effects, there are other possible
affects. Radiation-associated cardiac diseasesxvi
is known. Hypertension with its related cardiovascular diseases and
strokes has also been identified as associated with chronic exposure
to low-dose radiationxvii.
We
know that background radiation has health effectsxviii
but it seems that limited research has been conducted on diseases
other than cancer.
Many
of the residents of Port Hope, home to Canada’s uranium refinery
since
1933, feel that they have been “researched to death”xix
but
a
casual review of papers shows that many have time-lines that are too
short, populations sizes that are too small, and mixed outcomes which
do a disservice to all. Quantity
of research tells us nothing if it's poorly done.
Finally,
the myth believed by many physicians and the public is that we need
nuclear power for radioisotopes, for treatment or diagnosis. We do
not. We already make radioisotopes more safely in cyclotrons or
accelerators and could expand this to all medical radioisotopes.
In
conclusion, ionizing
radiation is not safe; nuclear power cannot be made safe. Physicians
have been altogether too silent about this industry – or, in fact,
silenced at
its very inception.
With the pressure on the government to support an industry that is
too slow, too costly and too dangerous to respond to the threatening
climate change, who
speaks for our great grandchildren?
iBurying
nuclear waste requires resources and uses energy as well –
currently high grade steel containers covered in copper have been
found to be the least likely to corrode. These do not seem to be
costed out in either monetary or environmental terms.
iiThe
half-life of plutonium-239 is 24,900 years; it takes ten half-lives
to disintegrate to almost unmeasurable amounts.
iiiThe
Nuclear Waste Management Organization (NWMO, pronounced “Noo-mo”)
was formed in 2002 by Canada’s nuclear electrical energy providers
as directed by the Nuclear Fuel Waste Act (NFWA). https://nwmo.ca
ivNWMO
engineers say that the containers won’t corrode because they are
made of the “finest steel” and covered with relatively
impervious-to-radiation copper. Does this mean that the tubing in
nuciear reactors is not the “finest steel”?
vhttps://www.theglobeandmail.com/canada/article-canada-nuclear-waste-management/
viFrom
Geosphere: A blog hosted by the European Geoscience Union. Note that
the graph starts at a “zero” of 1000 Bq.
https://blogs.egu.eu/network/geosphere/files/2014/12/Untitled.png
viihttps://www.choosingwisely.org/clinician-lists/american-academy-pediatrics-ct-scans-to-evaluate-minor-head-injuries/
viiihttps://nap.nationalacademies.org/resource/11340/beir_vii_final.pdf
ixP.
Kaatsch, C.Spix, S. Schmiedel, R. Schulze-Rath, A.Mergenthaler, and
M. Blettner, Epidemiologische Studie zu Kinderkrebs in der
Umgebung vonKerkraftwerken (KiKK Studie), Sltzgitter:
Bundesamp fuer Strablenschutz, 2007,
urn:nbn:de:0221-20100317939.
xhttps://www.sfgate.com/bayarea/article/Alice-Stewart-her-research-led-to-end-of-2800048.php
xii
J. A. Myrden, J. E. Hiltz, “Breast Cancer Following Multiple
Fluoroscopies During Artificial Pneumothorax Treatment of Pulmonary
Tuberculosis”, Canad. Med. Ass.J., June 14, 1969, vol 100
xiiiMark
J. Eisenberg, Johathan Afilalo, Patrick R. Lawler, Michal
Abramhamowicz, Hugues Righard, and Louise Pilot, “Cancr Risk
Related to Low-Dose Ionizing Radiation from Cardiac Imaging in
Patients after Acute Myocardial Infarction”, Canad. Med. Ass. J,
183(March 8, 2011); 430-436.
xivChinna
Babu Dracham, Abhash Shankar, and Renu Madan,”Radiation induced
secondary malignancies: a review article” Radiat Oncol J. 2018
Jun; 36(2): 85–94.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6074073/
xv
For
example: age
at radiation, dose and volume of irradiated area, type of irradiated
organ and tissue,
radiation
technique, individual and family history of cancer, chemotherapy,
cigarette-smoking, diet and
external
environment.
xviMilind
Y. Desai, “Radiation Associated Cardiac Disease”, American
College of Cardiology, June 21, 2017.
https://www.acc.org/latest-in-cardiology/articles/2017/06/13/07/13/radiation-associated-cardiac-disease
xviihttps://www.heart.org/en/news/2019/05/03/regular-low-level-radiation-exposure-raises-high-blood-pressure-risk
xviiiBen
Spycher, Judith Lupatsch, Marcel Zwahlen, Martin Roosli, Felix
Niggli, Michael Grotzer, Johannes Rischewski, Matthias Egger,
Claudia Kuehni, for the Swiss Pediatric Oncology Group and the Swiss
national Cohort Study Group, “Background Ionizing Radiation and
the Risk of Chilhood Cancer: A Census-Based Nationwide Cohort
Study”, Environmental Health Perspectives, June 1, 2015.
https://ehp.niehs.nih.gov/doi/full/10.1289/ehp.1408548
xixPersonal
communication with Port Hope citizen